Considering Change and Stasis Over Time in Indigenous Health History
June 21, 2026
Introduction
June is Indigenous History Month in Canada. While this can be a time to reflect on the past, it is also an opportunity to recognize how historical research can contribute to our understanding of the present. It offers an opportunity to explore the work of historians, including Indigenous health historians, whose research exposes the ongoing impacts of colonial policies and health systems, in turn pointing the way to new ways of thinking about and addressing gaps in health outcomes between Indigenous and non-Indigenous populations. By bringing these histories to light, health historians contribute to current conversations about health equity, reconciliation, and Indigenous well-being, demonstrating why this work is so vital today.
While it might seem counter-intuitive, historians, are not solely focused on a distant past that, while long over, might have some rippling residual impacts on the present. By taking a close look at what has changed, and what continues, historians can identify both past events that have a current impact, and issues that may have a long history, but are still happening. In their article “’Finally when I started falling down’: Indigenous tuberculosis patient experiences of health and illness on the Canadian prairies,” Abyoni et al write, “Despite the availability of effective medications, TB continues to persist in Indigenous communities, driven largely by Indigenous Peoples’ long history of enduring trauma, which continues to influence their contemporary experiences with TB and Its treatment.”[1] But careful historical analysis can tell us that trauma is not something that Indigenous people have endured in the past. In terms of Indigenous experiences with health care, traumatic experiences continue today. By identifying trauma as something in the past rather than something that is itself continuous, that is enduring, we miss an important opportunity to see Indigenous health outcome inequality through an historian’s lens, and through that lens to truly recognize and speak to Indigenous health inequality today.
The Manitoba Indigenous Tuberculosis History Project (MITHP) and its successor the Health and History Project (HHP) examine Indigenous experiences with western healthcare as a part of the work of understanding and addressing current issues in Indigenous health. For over a year now, these two projects have been tracking critical health care incidents involving anti-Indigenous racism that is documented in Canadian news media and in legal proceedings. Reading and following these stories has shown how important it is that, if we want to move away from these kinds of events and toward health equity, we must move away from thinking about critical incidents in health care involving anti-Indigenous racism as “one-offs” or discrete events that exist without or outside of any historical or cultural context or structure.
Seen as a collection, it is striking that there are so many current health care incidents involving anti-Indigenous racism. This is especially so given how difficult it is to document these stories. For one, the idea of systemic anti-Indigenous racism in health care goes against the prevailing logic that seeks to blame unequal health outcomes on Indigenous people. Added to this, for the people who have been harmed in these critical incidents, telling these stories to media, to lawyers, and to the courts, requires people to articulate and thus re-experience not only the actions and inactions of decision-makers with power over you and your care, but also the feelings of fear, anger and for some, self-doubt that go with them.[2] For many, it may be easier to try to put an incident behind them, but the feelings that stem from a critical health care incident involving anti-Indigenous racism aren’t so easily forgotten. Indigenous health history honours the stories of Indigenous people who have experienced critical health care incidents involving anti-Indigenous racism by helping to take this problem, and the hard-scrabble evidence of it, seriously, to help frame better understandings of its root causes, and to use those understandings to support anti-racism initiatives that can make a solid contribution to health care equality in Canada in the present.
Change and Continuity in Indigenous Tuberculosis History
A significant part of a historian’s work is to seek to understand change and continuity (sometimes called stasis) over time.[3] If we take the frame of Indigenous health, and measure across 100 years, that historical analysis reveals some incredibly valuable information, information that has significant implications for the present and future. Looking back, in 1930s Manitoba, the most concentrated and well-publicized health data about Indigenous people was centred around rates of death from tuberculosis (TB). In 1932, half of all people in Manitoba whose deaths were attributed to tuberculosis were First Nations, non-status Indians and Metis, even while together they represented only 5% of the population.[4]
Tuberculosis rates during the 1930s and 40s were also sometimes measured by “patient days,” the time a patient or group of patients spent in a particular sanatorium or hospital for TB treatment. This kind of data collection, however, did not distinguish between “White” and “Indian” patients the same way that other data that was collected by race did. It is possible that data collectors presumed that all patients in provincial hospitals were white and that hospital or sanatorium care was effectively closed to “Indians.” While this was not entirely true, the rates at which Indigenous people were taken to healthcare institutions for treatment in this period were much lower than for non-Indigenous populations. This changed, however, as TB treatment became far more effective in the middle of the 20th century, and white patient days dwindled. At the same time, armed with considerable coercive powers, Canada set its sights on waging war against a new enemy, “Indian TB.”
By 1950, medical professionals and government representatives could point to dramatic death rate declines depicted in bar charts and line graphs and reproduced in published TB reports. The following graph is typical of how TB data was collected and publicized during the years of the twentieth century when TB was most prevalent. From the 1930s to at least the 1960s, “Indianness” and “Whiteness” was the only factor depicted in these visual analyses of TB rates.
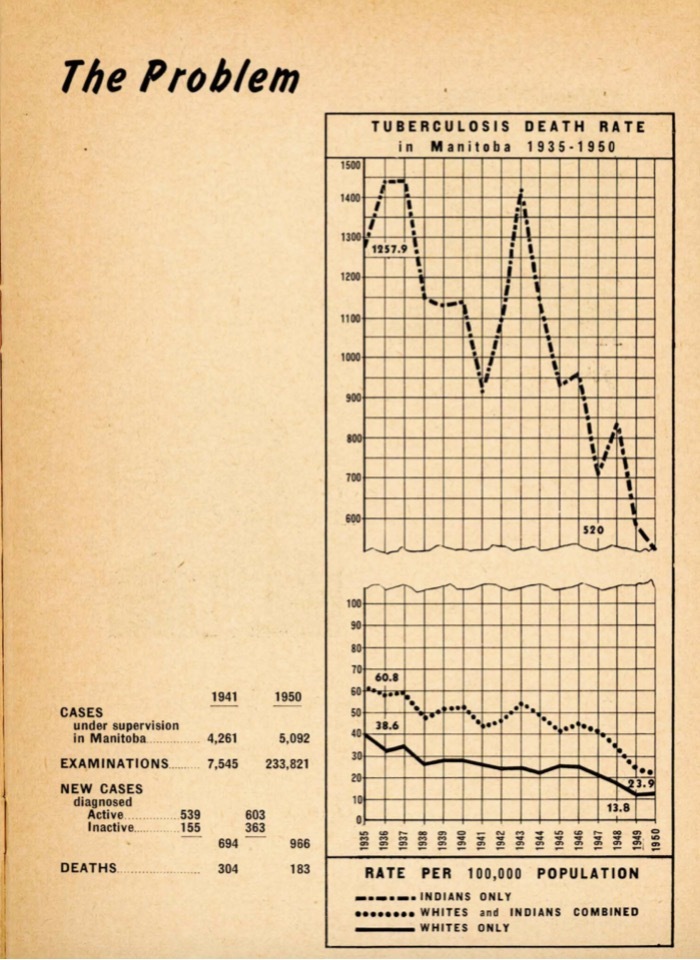
The top graph shows change over time in the number of “Indians” who died of TB each year, with the highest point being in 1937, showing1450 “Indians” dying of TB, to the lowest point of 520 “Indians” dying of TB in 1950. The bottom graph shows that the rates of death of “Whites and Indians Combined” is about 20/100,000 more than the death rate of “Whites Only.” To the Sanatorium Board of Manitoba, these graphs needed little explanation: they told “the story of the fight against tuberculosis.”[5] But the differentiation in statistics changed across time; in the 1930s, these kinds of statistics were used by physicians to build a case for extending TB treatment to First Nations because they were depicted as a “disease menace”[6] to white populations. By 1950, the differentiating statistic was a means to both celebrate and double-down on TB control mechanisms among First Nations, especially “preventative case-finding” (compulsory x-ray testing and removal of infections people from their communities to hospitals). What is interesting for this essay is that there is a narrowing of the gap between “Whites and Indians combined” and “Whites Only.” As historians, we are interested in that change, the narrowing of the gap, but also in its continuity, in the persistence of that gap itself.
It is very rare today to see tuberculosis death rate data; rather data on tuberculosis is commonly reported in terms of “incidence,” or the number people with new and active cases of tuberculosis per 100,000 people. By the mid-1940s, the Sanatorium Board of Manitoba included in its public reporting the numbers of “New Active Cases,” which became the standard “incidence” rate that remains in use today. New Active Cases in Manitoba for Whites in 1945 totalled 438 and in 1960, 218; for “Indians,” those numbers were 134 in 1945 and 66 in 1960. Manitoba’s Sanatorium Board celebrated the decline, and at the same time warned of a remaining “reservoir” of infection, referring to “tuberculous refugees from Europe” and First Nations.
Medical historians account for the lowering of tuberculosis death and incidence rates over time by pointing to highly successful innovations in TB case-finding and treatment including, starting in the 1940s, the use of x-ray technology in case-finding, and antibiotic treatment. But while advances in medical sciences and innovation reduced the size of the gap in tuberculosis incidence and deaths, the gap remains. If we look at the presence of a gap, we see continuity. In 2022, the TB incidence rate for all Canadians was 5.1 per 100,000, while the rate for First Nations was 21.4 per 100,000; in Manitoba, the rate across the province was 9.2 per 100,000 while the rate for First Nations only was 36.9 per 100,000.[7]
Historians can contribute to our understanding of this persistent gap between Indigenous and non-Indigenous health outcomes and what is happening with the ongoing margin after the limits of the capacity of innovations in medicine to narrow this gap have been reached. We do so by helping to gain a better understanding of the roots and persistence of health inequity in Canada.
As a group, MITHP and HHP have been and continue to be dedicated to caring about and for the Indigenous history of TB in Manitoba. Through our work, what we have learned is that Indigenous peoples’ history with tuberculosis is, in a way, a mirror of history in Manitoba: the unequal health outcomes Indigenous people face, including in tuberculosis are rooted in Indigenous experiences of violent, forced military and government- controlled colonization, violent dispossession, loss of land and resources, radically lived inequality imposed through the idea of white supremacy and Indigenous inferiority, and programs of economic favour and assimilation that enacted and maintained white supremacy at both high and every-day levels.
Enmeshed with this history, the concurrent rise of medical science and public health education in Canada means that these pasts are not separate. Our public health system is grounded in the concept that good patients, the type that deserve the best of care, look and act a certain way, that Indigenous people do not fit this model, and therefore do not deserve the same care as other Canadians. Unlike other citizens of Manitoba, Indigenous patient care is not a right subject to a known and equitable standard; rather it is a lived experience that derives from colonial motives that seek to protect white citizens whether from contagious illness or from a mirror that might reveal a less philanthropic side of itself to Canada, a mirror that might challenge comfortable narratives of uplift and assimilation as charitable acts.
This kind of health care does not need to be convenient or even humane; for many, medical treatments can require removal and transportation from home and considerable family disruption. Unlike other Manitobans, Indigenous people have and continue to experience health care as a system shaped by colonial priorities and unequal treatment where health policies function to protect settler populations. This lived reality challenges familiar national narratives that portray medical and social interventions as acts of benevolence and uplift. Beneath these narratives lies a health-care system that too often accepts Indigenous inconvenience, displacement, and even suffering as acceptable aspects of Indigenous health care, as medical intervention and treatment continues to require patients to be removed from their homes, families, languages, and communities, sometimes for extended periods of time, to health care institutions that continue to provide care rooted in historical pre-conceptions and prejudices.
The consequences of this reality, not just the echoes of past inequities, but rather a history that continues to manifest today, extend far beyond treatment regimes. Indigenous patients and their families have been and still are denied opportunities to understand medical decisions, participate in care, or remain connected with family and community during treatment. In cases of death, families have been left without timely information, unable to grieve properly, attend burials, or visit the final resting places of their loved ones. For many Indigenous people, western health care is associated with vulnerability, powerlessness, separation, and loss. These experiences continue to shape Indigenous relationships with western health care today. Understanding this history requires more than acknowledging past harms; it demands confronting the structures and assumptions that have normalized such treatment and recognizing how their effects continue to flow across and through generations. If Indigenous people have, and continue to, endure trauma, looking through an historian’s lens allows us to see that this is itself an enduring problem that continues to fuel the gap in health outcomes between Indigenous and white tuberculosis rates in Manitoba.
Conclusion
We can learn a lot about the present gap in Indigenous health and health outcomes when compared with the non-Indigenous population by studying Indigenous patient experiences over the past 100 years. As much as we may want it to, the persistent systemic racism in health care that we find won’t disappear overnight. By looking through a historian’s lens that identifies both change and continuity we see that, just as First Nations were regularly denied hospital care in the twentieth century, Black and Indigenous people face the longest Emergency Room wait times in Winnipeg Regional Health Authority and Health Sciences Centre today,[8] and are too often turned away without full and accurate medical assessment. Today, as in the past, Indigenous patients who experience, or who see their relations experience, systemic denial of care have reasonable concerns about quality of care and going to an institution that can’t be trusted to treat people equally. If we truly want to close the gap in health and health outcomes that persists in Canada today, health historians can help us identify the barriers that continue to work against this by considering the continuity of Indigenous experiences with health care that persists today.
[1] Abonyi, S., Mayan, M., Boffa, J., Lopez, C., McMullin, K., Heffernan, C., Hoeppner, V., King, M., Orr, P., & Long, R. (2017). “Finally when I started falling down”: Indigenous tuberculosis patient experiences of health and illness on the Canadian prairies. International Journal of Indigenous Health, 12(1), 3-24. Quoted in Regine Halseth and Omolara Odulaja, “Trauma-informed care in the management and treatment of Tuberculosis in Indigenous populations” (National Collaborating Centre for Indigenous Health, 2024), 6. Available at the National Collaborating Centre for Indigenous Health Website: https://www.nccih.ca/495/ Trauma-informed_care_in_the_management_and_treatment_of_Tuberculosisin_Indigenous_populations_.nccih?id=10445 Accessed 7 June 2026.
[2] Cheryle Dreaver, Rooted and Rising: Anti-Indigenous Racism Training in Action podcast, Season 1, episode 1, “What we learn. What we change,” First Nations Health and social Secretariat Manitoba, 1 June 2026 https://www.youtube.com/watch?v=EX62qhYr57k
[3] Winona Stevenson, “Decolonizing Tribal histories,” Ph D Dissertation, Univeristy of California Berkeley, 2000.
[4] Library and archives Council of Canada, Dominion Council of Health Fonds: Reel C-9815, “H.” D.A. Stewart, MD, Medical Superintendent [of Ninette Sanatorium], “Memorandum – Present views and facts re Tuberculosis among Indians in Manitoba,” 3.
[5] Tuberculosis Control in Manitoba 1950: Annual Report of the Sanatorium Board of Manitoba. Winnipeg, 1950, n.p.
[6] D.A. Stewart, “The Red Man and the White Plague,” Canadian Medical Association Journal 35, no. 6 (December 1936):674–75 and Maureen Lux, “Bacille de Calmette-Guerin, or BCG Vaccine for Tuberculosis,” Active History: History Matters 31 March, 2015, available at Activehistory.ca website, https://activehistory.ca/blog/2015/03/31/bacille-de-calmette-guerin-or-bcg-vaccine-for-tuberculosis/ Accessed 7 June 2026.
[7] Health Canada, “Tuberculosis in Canada: Epidemiological Update, 2022.” Available at the Government of Canada Website, https://www.canada.ca/en/public-health/services/publications/diseases-conditions/tuberculosis-canada-epidemiological-update-2022.html. Accessed 7 June, 2026.
[8] Shared Health Manitoba, Race, Ethnicity and Indigenous identity Data: Emergency Department Visits and Care Public Report June 2025. Available at Shared Health Manitoba website: https://sharedhealthmb.ca/wp-content/uploads/REI-Data-Public-Report-June-17-2025-2.pdf Accessed 7 June ,2026.